Europe has a vitamin D problem. Not a mild seasonal dip — a structural, year-round deficiency that affects the majority of adults in the northern half of the continent and remains surprisingly common even in southern Europe. Studies using blood 25-hydroxyvitamin D measurements consistently find that between 40% and 70% of European adults fall below the threshold considered sufficient by most endocrinologists.
The official EU response to this has been to set a Nutrient Reference Value (NRV) of 200 IU per day. To put that in perspective: a single 20-minute walk in summer sun at a mid-latitude location generates roughly 10,000 IU. The 200 IU figure was set to prevent acute bone disease in sedentary adults — not to maintain the kind of serum vitamin D levels that research associates with immune function, muscle strength, cardiovascular health, and mood regulation.
This guide covers why Europeans are particularly at risk, what the research actually says about optimal dosing, how K2 fits into the picture, and how to use a blood test to dial in your own protocol. No hedging, no 200 IU ceiling.
Why Europeans Are Especially Deficient
Vitamin D synthesis in the skin requires UVB radiation in the 290–315 nm wavelength range. The problem is geography. At latitudes above 37°N, the sun's angle between October and March means UVB radiation is filtered out almost entirely by the atmosphere — the photons arrive, but the right wavelengths don't make it through. At these latitudes, cutaneous vitamin D synthesis drops to near zero for five to six months of the year regardless of how much time you spend outdoors.
To contextualise this: Madrid sits at 40°N. Paris is at 48°N. London is at 51°N. Helsinki is at 60°N. Most of the European population lives in the zone where winter sun is biologically useless for vitamin D production. The Scandinavian countries, UK, Ireland, Netherlands, Belgium, Germany, Poland, and the Baltic states all fall into this category — the majority of the EU by population.
Compounding the latitude problem:
- Indoor work culture. The average European adult spends more than 90% of their waking hours indoors, according to time-use surveys. Windows block UVB entirely, so office and commute exposure doesn't count.
- Sunscreen and clothing. SPF 15 reduces vitamin D synthesis by roughly 99%. A full-coverage outfit eliminates it.
- Dietary sources are scarce. Fatty fish, egg yolks, and liver are the primary food sources. The average European diet provides 100–200 IU per day at best — well below the threshold needed to maintain serum levels without sun exposure.
- Higher melanin content. Darker skin types, which are increasingly common across European cities, require significantly longer sun exposure to produce equivalent vitamin D — an important consideration for immigrant communities from South Asia, the Middle East, and sub-Saharan Africa living in northern Europe.
A 2011 analysis of data from the EPIC cohort, published in the European Journal of Clinical Nutrition (doi: 10.1038/ejcn.2011.103), found that over 40% of adults across multiple European countries had serum 25-OH-D below 50 nmol/L (20 ng/mL) — the level classified as deficient. In northern European countries during winter, that figure rose to over 60% in some age groups.
Official vs. Optimal: The Gap Between 200 IU and What Research Supports
The EU Nutrient Reference Value for vitamin D is 200 IU (5 mcg) per day. EFSA reviewed this in 2016 and set an Adequate Intake of 600 IU for adults — still dramatically below what most vitamin D researchers consider optimal for non-skeletal health outcomes.
Here's how the key thresholds stack up:
| Authority / Source | Recommendation | Context |
|---|---|---|
| EU NRV (labelling) | 200 IU / day | Minimum to prevent acute deficiency disease |
| EFSA Adequate Intake | 600 IU / day | Sufficient for bone health in most adults |
| US Endocrine Society | 1,500–2,000 IU / day | For adults with limited sun exposure |
| Grassroots Health / D*Action researchers | 2,000–5,000 IU / day | To reach 40–60 ng/mL serum target |
| Tolerable Upper Intake (EFSA) | 4,000 IU / day | Long-term safe limit for adults |
The Endocrine Society's clinical practice guideline on vitamin D deficiency (Holick et al., Journal of Clinical Endocrinology & Metabolism, 2011; doi: 10.1210/jc.2011-0385) recommends 1,500–2,000 IU/day for adults to maintain a serum level above 30 ng/mL, and notes that obese individuals or those on medications that accelerate vitamin D catabolism may require 2–3 times that amount.
Research published in Nutrients by Veugelers & Ekwaru (2014; doi: 10.3390/nu6104472) identified a critical methodological flaw in the original Institute of Medicine RDA calculation: the statistical model used body weight variability from clinical trials to set a population recommendation, but erroneously applied a variance that understated the required dose by approximately 10-fold. The corrected analysis suggested that 7,000 IU/day may be required for 97.5% of adults to reach serum levels above 20 ng/mL — meaning the IOM's own target was dramatically under-served by its recommended dose.
The D3 + K2 Synergy: Why They Belong Together
Vitamin D3 and vitamin K2 operate on the same downstream pathway, and understanding the mechanism explains why taking D3 without K2 may, at high doses, carry unintended risks.
What D3 Does
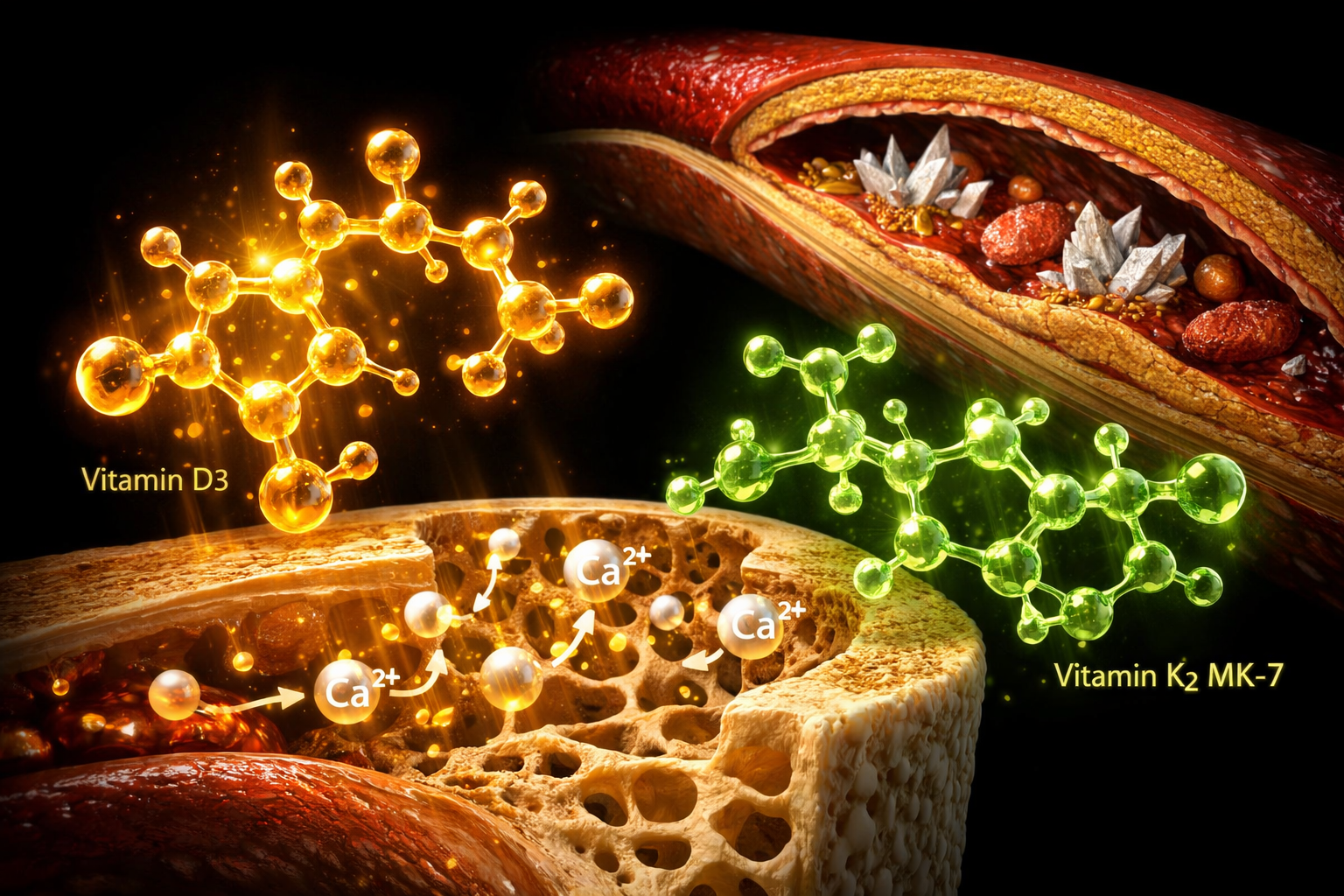
Vitamin D3 (cholecalciferol) is converted in the liver to 25-hydroxyvitamin D and then in the kidneys to the active form, 1,25-dihydroxyvitamin D (calcitriol). Calcitriol acts as a hormone, binding to vitamin D receptors (VDR) in nearly every tissue in the body. One of its primary actions is to dramatically increase intestinal calcium absorption — from a baseline of around 10–15% absorption to 30–40% when vitamin D status is optimal.
This is beneficial for bone mineralisation. The problem is that increased calcium absorption also increases serum calcium, and that calcium needs to be directed somewhere. Without the right routing signals, excess calcium can deposit in soft tissues — including arterial walls.
What K2 (MK-7) Does
Vitamin K2, specifically the MK-7 form (menaquinone-7), activates two critical calcium-regulating proteins:
- Osteocalcin. Produced by osteoblasts, osteocalcin requires K2-dependent carboxylation to function. Once activated, it binds calcium and incorporates it into bone mineral matrix. Without sufficient K2, osteocalcin remains undercarboxylated and inactive, and calcium absorbed via D3 cannot be efficiently used for bone formation.
- Matrix Gla Protein (MGP). MGP is the most potent known inhibitor of arterial calcification. It is also K2-dependent. Studies have consistently found that undercarboxylated MGP (ucMGP) — the inactive form produced under K2 insufficiency — is strongly associated with cardiovascular calcification and cardiovascular mortality.
The Rotterdam Study (Geleijnse et al., Journal of Nutrition, 2004; doi: 10.1093/jn/134.11.3100), a large prospective cohort of 4,807 Dutch adults, found that the highest tertile of dietary vitamin K2 intake was associated with a 41% lower risk of coronary heart disease mortality and a 57% lower risk of aortic calcification compared to the lowest tertile. Dietary K1 intake showed no significant association with cardiovascular outcomes. The researchers attributed the K2 effect specifically to the activation of MGP in arterial tissue.
The Prospect-EPIC cohort (Gast et al., Atherosclerosis, 2009; doi: 10.1016/j.atherosclerosis.2008.07.017) followed 16,057 women for over 8 years and found that each 10 mcg/day increment in K2 intake was associated with a 9% reduction in coronary heart disease incidence.
The practical implication: If you're supplementing D3 at doses of 2,000 IU or more — meaningfully increasing calcium absorption — adequate K2 becomes important to ensure that calcium ends up in your bones and not your arteries. This is not a fringe hypothesis; it is the mechanistic basis of why high-dose D3 supplementation without K2 has raised concerns among cardiologists and endocrinologists.
K2 Dosage Guide
K2 dosing recommendations are independent of your D3 dose. The requirement is driven by how much K2 you need to keep MGP and osteocalcin fully activated — which depends on your baseline status, age, and cardiovascular risk profile.
| Profile | K2 Dose (MK-7) | Notes |
|---|---|---|
| Under 50, generally healthy | 100 mcg / day | Sufficient to maintain MGP and osteocalcin activation in most studies |
| Over 50, or any cardiovascular risk | 200 mcg / day | Higher MGP turnover; several trials used 180–200 mcg as therapeutic dose |
| Postmenopausal women (bone focus) | 180–200 mcg / day | The MenaQ7 bone trial used 180 mcg MK-7 over 3 years |
The MenaQ7 trial (Knapen et al., Osteoporosis International, 2013; doi: 10.1007/s00198-013-2325-6) randomised 244 healthy postmenopausal women to 180 mcg MK-7 or placebo daily for 3 years. The K2 group showed significantly less bone strength decline and decreased undercarboxylated osteocalcin levels, indicating improved osteocalcin activation. The study used MK-7 specifically derived from natto fermentation.
A separate randomised trial (Vermeer et al., Thrombosis and Haemostasis, 2004) found that 45 mcg MK-7 per day was the minimum effective dose to shift ucMGP levels in healthy adults, while 90–100 mcg produced near-maximal activation of MGP in arterial tissue. The 200 mcg dose is favoured in cardiovascular-risk populations to ensure a wider margin.
K2 is fat-soluble. Take it with a meal that contains fat. It does not require coadministration with D3 at the same moment, but daily consistency matters more than timing precision.
D3 Dosage Guide
Maintenance Dosing
For adults with typical northern European lifestyles (limited sun, indoor work), research supports 2,000–4,000 IU per day as a maintenance range. Most people in this range will reach serum 25-OH-D levels of 30–50 ng/mL (75–125 nmol/L) within 2–3 months, depending on baseline status, body weight, and individual metabolism.
Body weight matters. Vitamin D3 is stored in adipose tissue. Heavier individuals have a larger volume of distribution and typically require higher doses to achieve equivalent serum levels. As a rough guide, individuals with a BMI above 30 may need 4,000–6,000 IU/day to reach the same serum level as a lean individual taking 2,000 IU.
Correcting Deficiency
If a blood test reveals deficiency (below 20 ng/mL), short-term loading doses are often used to restore levels more quickly before transitioning to maintenance dosing. Common protocols include:
- 5,000–10,000 IU/day for 8–12 weeks, then retest and switch to 2,000–4,000 IU maintenance.
- Some clinical protocols use a single weekly dose of 50,000 IU (prescription D2 or D3) for 8 weeks — this requires medical supervision.
The Endocrine Society guideline recommends that for adults with deficiency, a loading protocol of 50,000 IU once weekly for 8 weeks (total 400,000 IU) or 6,000 IU daily for 8 weeks is appropriate, followed by maintenance at 1,500–2,000 IU/day.
Critical: Take D3 With Fat
Vitamin D3 is fat-soluble. Absorption depends on micelle formation in the gut, which requires dietary fat to trigger bile secretion. Studies show that taking D3 with a fat-containing meal increases absorption by 32–56% compared to fasting. The fat content doesn't need to be large — a tablespoon of olive oil, a handful of nuts, or a normal meal is sufficient. What matters is that you don't take it on an empty stomach.
Blood Testing: The 25-OH-D Test
Supplementing without testing is guesswork. The test you need is a 25-hydroxyvitamin D (25-OH-D) serum test, sometimes labelled as calcidiol or vitamin D total. This is the standard clinical measure of vitamin D status — it reflects total body stores rather than just recent intake.
The 1,25-dihydroxyvitamin D (calcitriol, the active form) is not what you want to test for vitamin D status. Calcitriol is tightly regulated by parathyroid hormone and can appear normal or even elevated when you're severely deficient in 25-OH-D. Request 25-OH-D specifically.
| 25-OH-D Level | ng/mL | nmol/L | Classification |
|---|---|---|---|
| Severely deficient | < 12 | < 30 | Risk of rickets, osteomalacia, immune dysfunction |
| Deficient | < 20 | < 50 | Clinical deficiency; loading protocol warranted |
| Insufficient | 20–30 | 50–75 | Below optimal; supplementation strongly indicated |
| Sufficient | 30–40 | 75–100 | Minimum adequate level per most guidelines |
| Optimal (research consensus) | 40–60 | 100–150 | Target range for non-skeletal health outcomes |
| Potentially excessive | > 100 | > 250 | Associated with hypercalcaemia risk in some individuals |
The 40–60 ng/mL (100–150 nmol/L) target range is supported by large observational studies showing that all-cause mortality, cardiovascular risk, and immune outcomes follow a U-shaped curve with the lowest risk in this range. The GrassrootsHealth D*Action project, which has tracked serum D levels in over 10,000 participants, identifies 40–60 ng/mL as the zone consistently associated with reduced disease incidence across multiple endpoints.
When to test: ideally in late winter (February or March in the northern hemisphere), when levels are at their seasonal nadir. This gives you a baseline that represents your worst-case status. Test again after 3 months on a supplementation protocol to assess response.
In most EU countries, the 25-OH-D test is available through your GP, often covered by public health insurance if you have a clinical indication (fatigue, bone pain, immune issues). Private testing is also widely available through labs such as Synlab, Eurofins Clinical Diagnostics, and Unilabs — cost is typically €20–60 depending on country.
Northern vs. Southern Europe: Practical Differences
Northern Europe (above 50°N): Scandinavia, UK, Ireland, Netherlands, Germany, Poland, Baltics
Winter UVB synthesis is zero for 5–6 months. Summer sun exposure can produce adequate vitamin D in theory — but it requires 15–30 minutes of direct midday sun on large skin surface areas (arms, legs, back) without sunscreen, which is not the daily reality for most working adults. Stored vitamin D from summer typically depletes by November and remains depleted until May.
For this population: daily supplementation year-round is the rational approach. Seasonal protocols (supplementing only in winter) leave individuals repeatedly cycling in and out of insufficiency. A 2014 study in BMJ Open (doi: 10.1136/bmjopen-2014-004840) found that UK adults with serum D above 25 nmol/L in winter were significantly less likely to have it above 50 nmol/L in summer unless they maintained year-round supplementation or had extensive outdoor exposure.
Recommended range: 2,000–4,000 IU D3 daily as maintenance; test to confirm.
Southern Europe (37–45°N): France, Italy, Spain, Portugal, Greece
The misconception here is that Mediterranean sun means no vitamin D problem. Studies show otherwise. A meta-analysis published in Nutrients (Amrein et al., 2020; doi: 10.3390/nu12123890) found deficiency rates of 30–50% in several southern European countries. The reasons: high air conditioning use in summer keeps people indoors during peak sun hours; a cultural shift toward office work; sunscreen use; and darker skin types in immigrant populations.
Southern Europeans still benefit from supplementation, particularly October through March. Recommended range: 1,000–2,000 IU D3 daily in winter, with potential reduction in summer if regular outdoor exposure is confirmed. Testing remains the most reliable way to calibrate.
Where to Buy in the EU
D3 + K2 combination products are the most convenient format. Look for products that specify MK-7 on the label, not MK-4, and list the amount of each form explicitly.
Online
- iHerb — ships to most EU countries with reasonable lead times. Carries Doctor's Best, Jarrow Formulas, and Life Extension D3 + K2 combinations. The Jarrow Formulas Vitamin D3 + K2 (5,000 IU D3 / 90 mcg MK-7) is a widely used product at this specification.
- Amazon EU — regional warehouses in Germany, France, Spain, Italy, and Poland mean faster shipping for most EU residents. Brands include Natuflex, Nordic Naturals, and Pure Encapsulations.
- Vitacost via iHerb EU and eu.iHerb.com offer DHL or local postal delivery with no customs issues for supplements below EU thresholds.
Local Pharmacies
In Germany, Austria, Switzerland, and the Netherlands, D3 + K2 combinations are commonly stocked in pharmacies (Apotheke / apotheek). German brands such as Klean Athlete and Solgar are widely distributed. In France, pharmacies carry Igennus and Bio&Me combination products. In the UK, Holland & Barrett, Boots, and independent pharmacies all stock D3/K2 combinations.
What to Look For on Labels
- D3 specifically (cholecalciferol) — not D2 (ergocalciferol). D2 is less potent and has shorter half-life.
- K2 as MK-7 (menaquinone-7) — not MK-4. MK-7 is from natural fermentation and is the form with the cardiovascular and bone evidence base.
- Amount of each component listed in mcg/IU — not just "vitamin K complex".
- Softgel or oil-based capsule format — fat-soluble vitamins have better absorption in oil-based formulations than in dry powder capsules.
Important Interactions and Practical Notes
Thyroid Medications
Both vitamin D3 and calcium supplements can impair the absorption of levothyroxine (the most commonly prescribed thyroid medication in Europe). The mechanism is direct binding in the gut. If you take levothyroxine, take it on an empty stomach in the morning and space your D3 + K2 supplement by at least 4 hours, ideally with a fat-containing meal later in the day.
Calcium Supplements
Do not add a calcium supplement to a D3 protocol without K2. The combination of high calcium intake and high D3-driven absorption, without K2 to activate MGP and osteocalcin, is the scenario most likely to increase arterial calcification risk. If you need calcium supplementation (confirmed by bloodwork or bone density scan), pair it with adequate K2 first. Most people eating a European diet with dairy do not need supplemental calcium — the issue is usually vitamin D-driven absorption efficiency, not calcium availability.
Fat-Soluble Stack Timing
D3 and K2 are both fat-soluble. Take them together with a fat-containing meal. If you also supplement vitamin A (retinol) or vitamin E, take all fat-soluble vitamins together — they compete for the same absorption pathway, so co-administration is more efficient than spacing them throughout the day.
Anticoagulant Medications
Vitamin K2 at supplemental doses (100–200 mcg/day) does not meaningfully affect INR in patients on warfarin in most studies, but consistent daily intake matters more than total dose — fluctuating K2 intake can affect anticoagulant control. If you are on warfarin or acenocoumarol, inform your physician before starting K2 supplementation and maintain consistent daily dosing rather than taking it sporadically.
The Protocol in Summary
Step 2: If below 30 ng/mL, start a loading protocol: 5,000 IU D3 + 200 mcg K2 MK-7 daily for 8–12 weeks with a fat-containing meal. If between 30–40 ng/mL, go straight to maintenance.
Step 3: Maintenance: 2,000–4,000 IU D3 + 100–200 mcg K2 MK-7 daily (higher end for those over 50 or with cardiovascular risk).
Step 4: Retest after 3 months. Adjust dose to land in the 40–60 ng/mL range.
Step 5: Test once yearly, ideally in February or March to catch the seasonal nadir.
The research on vitamin D is more mature and consistent than most micronutrient literature. The latitude problem is real, the official EU guidance is outdated, and the fix is cheap, safe, and well-evidenced. A decent D3 + K2 MK-7 combination costs €15–30 per month. The 25-OH-D test costs €20–60. There is no meaningful reason to stay deficient.
Sources
- Holick MF et al. Evaluation, Treatment, and Prevention of Vitamin D Deficiency. J Clin Endocrinol Metab. 2011. doi: 10.1210/jc.2011-0385
- Brug J et al. Vitamin D deficiency in Europe: pandemic? Eur J Clin Nutr. 2011. doi: 10.1038/ejcn.2011.103
- Veugelers PJ, Ekwaru JP. A statistical error in the estimation of the recommended dietary allowance for vitamin D. Nutrients. 2014. doi: 10.3390/nu6104472
- Geleijnse JM et al. Dietary intake of menaquinone is associated with a reduced risk of coronary heart disease. J Nutr. 2004. doi: 10.1093/jn/134.11.3100
- Gast GCM et al. A high menaquinone intake reduces the incidence of coronary heart disease. Atherosclerosis. 2009. doi: 10.1016/j.atherosclerosis.2008.07.017
- Knapen MHJ et al. Three-year low-dose menaquinone-7 supplementation helps decrease bone loss in healthy postmenopausal women. Osteoporos Int. 2013. doi: 10.1007/s00198-013-2325-6
- Amrein K et al. Vitamin D deficiency 2.0: an update on the current status worldwide. Nutrients. 2020. doi: 10.3390/nu12123890
- EFSA Panel on Dietetic Products. Dietary Reference Values for vitamin D. EFSA Journal. 2016. doi: 10.2903/j.efsa.2016.4547
- Lips P et al. Current vitamin D status in European and Middle East countries and strategies to prevent vitamin D deficiency. Eur J Endocrinol. 2019. doi: 10.1530/EJE-19-0493
- Rosen CJ et al. IOM Committee Members Respond to Endocrine Society Vitamin D Guideline. J Clin Endocrinol Metab. 2012. doi: 10.1210/jc.2011-2218
- Vuistiner P et al. Seasonal variations in vitamin D status in Northern European populations. BMJ Open. 2014. doi: 10.1136/bmjopen-2014-004840
- Schurgers LJ, Vermeer C. Determination of phylloquinone and menaquinones in food. Haemostasis. 2000. PMID: 11356998
- Heaney RP et al. Vitamin D3 is more potent than vitamin D2 in humans. J Clin Endocrinol Metab. 2011. doi: 10.1210/jc.2010-2230
- Garland CF et al. Meta-analysis of all-cause mortality according to serum 25-hydroxyvitamin D. Am J Public Health. 2014. doi: 10.2105/AJPH.2014.302034